
While intramuscular administration of Testosterone has been shown to be a very effective delivery method for trans men, research suggests that 40% of those who received IM injections described it as very painful. (Najafidolatabad, 2010.)
Are there ways to reduce the pain associated with IM Testosterone injections? A Google search or Facebook post will yield all kinds of conflicting information. This review of scientific studies sets the record straight on minimizing post-injection pain from IM injections.
To minimize post-injection pain, several important factors need to first be considered:
- Injection site
- Needle length, gauge, and “switching up”
- Volume of injection
- Injection technique, including speed of injection
- Massage and manual pressure
Injection Site
With IM injections, Testosterone is deposited deeply into vascular muscle tissue. The deltoid (arm), vastus lateralis (thigh), and gluteal muscles (hip/buttocks) are the most common sites for IM injections.
Some injection sites are more prone to pain than others. Areas of the body with less subcutaneous fat are generally less painful injection sites.
The ventrogluteal site has less subcutaneous tissue and a thicker muscle mass than the dorsogluteal site. Therefore, the needle has a better chance of reaching the muscular tissue in the ventrogluteal area than in the dorsogluteal area. In various studies it was found that most injections given to the dorsogluteal site delivered medication into the fatty tissue. Pain receptors are found within the subcutaneous layer, not in muscle tissues and so injections administered into subcutaneous tissue may be more painful. (Güneş, 2013.)
Rotating injection sites is a must! Give an injection site a week or two off before injecting there again. This helps to limit injection site reactions and the formation of scar tissue.
It has been found that necrosis of the muscle will occur after any IM injection no matter what medication is injected. The only variable is the size of the necrotic lesion and the severity of it. Forceful placement of a volume of fluid into a closed space will cause damage. In other words, the surrounding muscle and tissues in the immediate area of the needle tip are subjected to the pressure of the mass of fluid that has been instilled into the area, which causes pressure necrosis. The toxicity of the medication, the volume injected, and even the speed at which the injection is given also will influence the size of the necrotic lesion. (Treadwell, 2003)
Needle Length, Gauge and “Switching Up”
The needle used to inject should be long enough to penetrate through the subcutaneous tissue into the muscle mass, or the patient will have more pain. (Güneş, 2013.) The typical needle gauge used to inject testosterone is between 22 and 25. It would stand to reason that using a smaller gauge needle would reduce injection pain, but researchers have disagreed on this on this point. (Gill, 2007 and Flanagan, 2007.)
Just Say No to Blunts! Trans men are commonly advised to use one needle for drawing up, discard it, and then “switch up” to a higher gauge needle for injection. Here’s why:
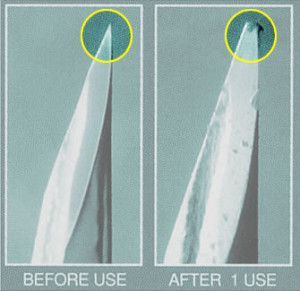
It’s not hard to imagine that the duller tip of the needle would cause more pain, but again, studies have not unanimously concluded that this is the case (Rock, 2000 and Ağaç, 2011.)
Volume of Injection
The volume of injection can contribute to post-injection pain. Smaller, more frequent injections are likely to cause less pain than larger injections administered bi-weekly (or every few months in the case of long acting T. preparations like Nebido.)
Injection Technique
Injection technique is another consideration when evaluating post-injection pain, but research in this area is also conflicting. In one study, the Air-lock (AL) injection technique was found to be more effective at reducing pain caused by IM injection versus the Z-track (ZT) method (Najafidolatabad, 2010.) Earlier studies also found AL was a better method for avoiding seepage of the medication, which is associated with lower absorption and pain (Quartermaine, 1995 and Mac Gabhann 1998.) On the other hand, other studies from the ’80s found the opposite to be true, that Z-track is associated with less post-injection pain (Keen, 1986 and Kim, 1988.)
Katsma and Smith (1997) suggested that the potential for pain with IM injections is due to the kinematics of injections (the movement of the needle through muscle and tissue) and concluded that, “minimizing of this effect is accomplished by controlling the needle trajectory during penetration along a linear path from point of contact to end point.” In other words, the needle should go straight in, with no deviations in its path.
Does injection speed play a role in post-injection pain? Again, it’s hard to say: two studies concluded that injection speed was not a factor (Mitchell, 2001 and Chan, 2001) while a more recent study showed that faster injections induced less pain in babies (Lundberg, 2008.)
To Massage or Not to Massage?
There are different injection protocols for different medications, so advice you find online about this may or may not apply to your Testosterone injection. For example, with the IM injection of vaccines, massaging the site of injection is highly discouraged as it can push the medication into the subcutaneous layer, reducing effectiveness and potentially causing irritation.
Given that subcutaneous administration of Testosterone has been proven effective why would the migration of T. into the subcutaneous layer be problematic? Because pain receptors are in the subcutaneous layer not in muscle tissue (Güneş, 2013.) Massaging the injection site can push the T. into the subcutaneous layer where there is greater sensitivity to pain.
Discussions on nursing forums, as well as journal articles, indicate that massaging the injection site is an out-of-date technique (Beyea, 1995.) Indeed, the Australian Immunisation Handbook, a critical nursing reference now in its 10th edition, had advised against rubbing IM injection sites, and the recommendation to “gently apply pressure for 1 or 2 minutes” post-injection does not appear in the latest edition.

“Oh people can come up with statistics to prove anything, Kent. Forty percent of all people know that.” – Homer Simpson
However, the findings of a 2001 study indicated that massage was effective in reducing pain perception of adult patients after the administration of an intramuscular injection.
Even with evidenced-based research, it’s hard to know what’s actually true!
What about applying pressure before an injection? A 1996 study found that this lessened post-injection pain. Subjects in a 2002 study reported also lower pain intensity scores with manual pressure applied before injections, suggesting that this could be an effective means of decreasing post-injection pain (Chung, 2002.)
With the science out of the way, let’s get down to the practical things you can do to improve your IM injection experience!
10 Tips to Reduce IM Injection Pain (YMMV)
1. Find injection sites that work for you (“sweet spots”) and rotate them. The deltoid (arm), vastus lateralis (thigh), and ventrogluteal (hip/butt) muscles are acceptable sites for IM injections. The common dorsogluteal injection site is no longer recommended. (Doing T shots in your butt? Read this.)
2. Choose your gear wisely. Use a needle that is long enough to penetrate deep into the muscle. Use a larger gauge needle for drawing up, then switch to a smaller gauge needle to inject.
3. Shorten your cycle. If you’re injecting every 14 days, you might try moving to a 7 day cycle to see if injecting the smaller volume helps minimize pain.
4. Re-visit your injection technique. Air-lock or Z-track? Are you injecting straight in or does the trajectory of the needle shift during injection? Fast or slow? Small tweaks to your technique might provide big wins in reducing post-injection pain.
5. Warm up and relax. Have a hot shower or bath before your injection to warm up the injection site. While injecting, keep the muscle relaxed (and unflexed.)
6. Warm up your T. too! Hold the vial in a closed fist for a couple of minutes, run it under hot water or place it on a baseboard heater for a minute to warm the T. to room temperature or a little higher. Warm oil in a warm muscle will produce less pain than cold oil in a cold muscle!
7. After sterilizing the injection site with alcohol, let the skin dry. Penetrating the skin with the needle before the alcohol has evaporated can cause a stinging pain sensation.
8. Apply manual pressure to the injection site for 10 seconds before your injection. Be sure to maintain sterility!
9. After your injection, reduce pain and swelling by applying topical Arnica gel or cream, and then ice the injection site.
10. Some people swear by it, so massage the site after injection if you think it helps!
Pain after an IM Testosterone injection is very common but there are numerous things you can do to minimize and even eliminate post-injection pain. In the end, every body is different and what works for one guy may not work so well for another. So, knowing that science doesn’t have all the answers yet, just do what works for YOU to maintain pain-free injections!
Also see: Subcutaneous Administration of Testosterone Safe, Effective Alternative to IM Injections
References
Najafidolatabad SH, Malekzadeh J, Mohebbinovbandegani Z. Comparison of the pain severity, drug leakage and ecchymosis rates caused by the application on tramadol intramuscular injection in Z-track and Air-lock Techniques. Invest Educ Enferm. 2010; 28(2):171-175
Ülkü Yapucu Günes, Dilek Kara, Suer Ari, Onur Ceyhan. Which site is more painful in intramuscular injections? The dorsogluteal site or the ventrogluteal site? A case study from Turkey
Clinical Nursing Studies, Vol 1, Num 4 (2013)
Terry Treadwell, MD, FACS. Diagnostic Dilemma: Intramuscular Injection Site Injuries Masquerading As Pressure Ulcers. WOUNDS. 2003;15(9):302-312.
Harvinder S. Gill and Mark R. Prausnitz. Does Needle Size Matter? J Diabetes Sci Technol. 2007 Sep; 1(5): 725–729.
Flanagan T, Wahl MJ, Schmitt MM, Wahl JA. Size doesn’t matter: needle gauge and injection pain. Gen Dent. 2007 May-Jun;55(3):216-7.
Rock D. Does drawing up technique influence patients’ perception of pain at the injection site? Aust N Z J Ment Health Nurs. 2000 Sep;9(3):147-51.
Agaç E, Günes UY. Effect on pain of changing the needle prior to administering medicine intramuscularly: a randomized controlled trial. J Adv Nurs. 2011 Mar;67(3):563-8. doi: 10.1111/j.1365-2648.2010.05513.x.
Quartermaine S, Taylor R. A comparative study of depot injection techniques. Nurs Times. 1995 Jul 26-Aug 1;91(30):36-9.
Mac Gabhann L. A comparison of two depot injection techniques. Nurs Stand. 1998 Jun 3-9;12(37):39-41.
Keen MF. Comparison of intramuscular injection techniques to reduce site discomfort and lesions. Nurs Res. 1986 Jul-Aug;35(4):207-10.
Kim KS. Kanho Hakhoe Chi. [Comparison of two intramuscular injection technics on the severity of discomfort and lesions at the injection site]. [Article in Korean] 1988 Dec;18(3):257-68.
Katsma D, Smith G. Analysis of needle path during intramuscular injection. Nurs Res. 1997 Sep-Oct;46(5):288-92.
Mitchell JR, Whitney FW. The effect of injection speed on the perception of intramuscular injection pain. A clinical update. AAOHN J. 2001 Jun;49(6):286-92.
Chan H. Effects of injection duration on site-pain intensity and bruising associated with subcutaneous heparin. J Adv Nurs. 2001 Sep;35(6):882-92
Lundberg GD. Rapid Injections Trump Slow for Minimizing Injection Pain. The Medscape Journal of Medicine. 2008;10(3):62
Beyea SC, Nicoll LH. Administration of medications via the intramuscular route: an integrative review of the literature and research-based protocol for the procedure. Appl Nurs Res. 1995 Feb;8(1):23-33
Kanika, K Helen Rani, Shobha Prasad. Effect of massage on pain perception after administration of Intramuscular Injection among adult patients. Nursing and Midwifery Research Journal, Vol-7, No. 3, July 2011
Barnhill BJ, Holbert MD, Jackson NM, Erickson RS. Using pressure to decrease the pain of intramuscular injections. J Pain Symptom Manage. 1996 Jul;12(1):52-8.
Chung JW, Ng WM, Wong TK. An experimental study on the use of manual pressure to reduce pain in intramuscular injections. J Clin Nurs. 2002 Jul;11(4):457-61.

This is an excellent, thorough review of the info out there on IM injections for T. I would add to this to talk to your healthcare provider about the possibility of switching to subcutaneous injections. Many younger trans male teens start out with subcutaneous injections, and stick with that method because it’s less painful: you can use a smaller needle tip, inject into a fatty area like the belly (less painful than injecting into muscle), and you don’t have to rotate injection sites. I was working with these kids when I started T, and asked my doctor if there was anything stopping me from injecting subcutaneously instead of intramuscularly. 4 years later and I am still injecting once a week subcutaneously, with all the physical changes I want, and of course monitoring my hormone levels with my doctor twice a year. Everyone needs to find the right technique for their own hormone delivery, but I wish other trans men were informed by their healthcare providers that there is a less painful option out there that might work for them.
Thank you! Yes! Sub-q is definitely growing in popularity. I didn’t go into detail about it because this article is about making the IM experience better, not about other delivery methods.
Pain receptors are in that sub-q layer, not in muscle, so I find it surprising that sub-q scores as well as it does on post-injection pain. Studies indicate that one of the reasons is because sub-q injections are lower volume. Makes sense.
Another factor in terms of volume is the concentration of T. In Canada, a 200mg/ml concentration is almost twice as expensive as 100mg/ml. So, if one doesn’t have access to a higher concentration T., and prefers less frequent injections, IM is indicated.
That said, it’s rare for sub-q to be offered as an option! The “IM only” warning on T. leaflets doesn’t help spread the good word, but recent studies are getting it across.
Great article to help us understand what we can improve or add to ensure a smooth injection process. Can you provide a glossary of some of the technical/medical terms used? I got a bit lost and confused as I was reading it. I want to make sure I absorb all the information and understand it correctly. Laypersons’ terms in brackets after technical terms would really help. Thanks for all your work and help compiling and report.
Thank you Kai! I added some links to explain airlock vs. z-track techniques, and kinematics. Anything else in particular that I can clarify?
Do I need to pinch the skin first then inject or make the skin tight in the thigh before injecting. I’m a little confused on that part. Does it affect the process or slow it down any?
There are lots of different methods for IM injections. I don’t pinch or make the skin tight. Do what works for you.
I read someplace that making the skin as taught as possible reduces any sticking sting… Seems to work for me but I’m a chicken when it comes to injection time. Sticking a needle into my body just seems a contradiction to common sense.
The needles i have for testosterone the only ones i can get are 0.8 x25ml can i use them. What problems will i have if any or how should i use them.
Can I ask, not to get anyone in trouble, but is the only way to get a hold of actual testosterone thru a physician? I know it’s prescribed, but for me, I can’t pursue that really.
I’ve tried to befriend guys at the gym, who could possibly have access to roids, but that’s not panned-out to get me connected. It’s a difficult thing to explain, but i’m not a Trans-male, but someone who was born with a condition called Klinefelter Syndrome, meaning I was born male, but later learned I was born with an extra X chronsome, and it puts me on the XXY gender spectrum. About 1 in 500 male births qualify as XXY. I’m of normal intelligence, though people with the disorder tend to be of less-than-average IQs,and have a feminine body for a man, and had gynecomastia and removal surgery for that. It’s been a very difficult road for me, and, as you can imagine, it’s a difficult life to manage. To sort of weirdly complicate my own life, I only ever attended boy’s Catholic schools, so, you can guess how that played out. I often have been mistaken for a girl, and have had the three-times-repeated experience of being at a gay bar, and asked if I was a trans-woman, meaning that I was born and raised as a woman, but transitioned to a male appearance. It’s odd then, when i’ve wanted to become more male in appearance. I have low testosterone, but that is not something you can ask a doctor to help you resolve. They don’t seem to get it, and it’s incredibly hard for me to pursue myself. And I want to be in control of my own body, and not given a thumbs-up or thumbs-down, or suffer through the process of constantly being under the microscope. And then as a gay man, who does not look “GQ-ready”, is a terrible thing to go through. I turned to you guys, I guess because you could sort of relate. Thanks and thanks for listening.
You can certainly ask, Daniel. Hormone therapy is a standard treatment for Klinefelter Syndrome. https://www.nichd.nih.gov/health/topics/klinefelter/conditioninfo/Pages/treatments.aspx
Have you ever seen an endocrinologist for KS? After confirming low testosterone and hearing about your needs, they would most likely prescribe Testosterone.
You would need a referral from your primary care provider. If you don’t have a PCP, you could called Planned Parenthood centers near you that offer LGBT services and they may be able to help or point you in the right direction.
https://www.plannedparenthood.org/health-center/MO
While I can understand the desire to pursue this without a doctor, that is really the safest way to proceed. Aside from legal issues, you would know exactly what you are buying, which can’t be said of underground labs that sell hormones to bodybuilders, and you would have a regular supply, which would be better for your health.
I hope this helps!
Hi Jamie, it sounds like a 21 gauge, 1″ (length) needle. The gauge could be smaller, but 21 isn’t too big. The 1″ length could be problematic depending on subcutaneous fat:
“Thickness of fat in this area… One study found the success rate of IM injections to be 32% (which fell to 8% in female patients)!”
Source: Common T Injection Site No Longer Recommended
Loved the article but i have to disagree with you on one thing and that’s injecting in the fat is more painful. For me personally, i dont even feel the needle go in (using my outer thigh fat) whereas when i tried injecting into the muscle sometimes I’d clench/flex after the injection – that hurt a bit. Not saying it’s the same for everyone of course.
I never thought about warming up my T though! My place is chilly so thats a good idea to hold it in my hands for a while. Maybe keep it wrapped in power towel or something?
Thanks for posting this.
I don’t feel a thing when i inject into my outer thigh fat.
Drawing up: 18g, 1 1/2 inches
Injecting: 23g, 1 inch
Testosterone vial: 1000mg
Can you inject into the shoulder muscle instead of bicep or thigh??? I use a 20 guage needle and it’s a inch and half long. A little big but It don’t hurt. I inject in my shoulder muscle. What do you think???
Yup, deltoid: http://www.spotinjections.com/delt1.htm
I would use a 1″ needle though. And you can go to a smaller guage too; I like 22.
Sorry it’s a one inch needle!
This article mentions ice after a shot but what about before? Is it okay to ice an injection site prior to injecting?
Why not just go trice weekly subq
Thank you for your tip to take a shower or bath before injecting yourself with the testosterone. My brother has been wanting to start on testosterone, so I was looking up some tips to help with injecting. I will make sure to keep this tip in mind so that I might help him as much as possible.
Too be honest, I am not transgender. However, I have read a couple of these articles after having pain from IM injections of Sustanon 250. I have taken it for a while now as I’m getting older and the persistent pain as of late has me seeking answers. Two of your articles have been extremely helpful. I hope it’s ok I went through this and commented. Thank you for the insight.
Super glad the info helped you out, Rich!
Imo some massage is helpful to avoid encapsulation, too much would be adverse because it could make for a faster uptake into the bloodstream. And it may help make it a bit less painful. A middle ground might be a good solution.